The Alameda study gave us seven habits of healthy people
- Avoiding snacks
- Eating breakfast regularly
- Exercising
- Maintaining desirable weight for height
- Not smoking
- Drinking less than five drinks in one sitting
- Sleeping 7-8 hours a night
These seven habits can be divided into three major categories: Eat well, Be Active and Smoke-Free, and Minimize Drinking.
Eat Well:
Our bodies require 46 nutrients to remain healthy. Water is essential to transport nutrients through the bloodstream, remove wastes, and regulate the body’s temperature. Although need varies by individual, most people stay well hydrated with eight 8-oz glasses of water a day. You will know you are drinking enough if you need to pee every two to four hours and the urine is a light color. The other nutrients are divided into five categories: proteins, fats, carbohydrates, minerals, and vitamins.
The U.S. Department of Agriculture suggests dividing your plate into five food groups with approximately 30% vegetables, 30% grains, 20% fruits, 20% protein, and a small circle of dairy. What you eat is just as important as what you don’t eat. Try to buy and eat foods that are minimally processed. The best way to do this is to shop the outskirts of the grocery store. You’ll notice that the outskirts tend to be the fresher, less processed foods.
Here are some power foods that are loaded with nutrients:
- Low-fat Yogurt
- Eggs
- Nuts
- Kiwi
- Quinoa
- Beans
- Salmon
- Broccoli
- Berries
If you want to read more about recommended diets, check out:
https://www.choosemyplate.gov/

Be Active and Smoke-Free
Adults should engage in 150 minutes of moderate intensity or 75 minutes of high-intensity activity per week. This activity can be a combination of 10-minute episodes spread through the week. The guidelines also suggest muscle-strengthening activities for all muscle groups at least twice a week. You have 10 minutes a day to dedicate to your health, right? Physical activity not only reduces mortality from different diseases but also increases life expectancy, improves cardiovascular recovery from stress. Psychologically, physical activity has been correlated with reduced symptoms of depression, less anxiety, and increased self-esteem.
Cigarette smoking is the most preventable cause of illness, disability, and premature death in the United States. A lit cigarette releases 4000 different chemicals into the body. Smoking is also a cause of cancer, causes an increased risk of dementia, and can contribute to the development of cardiovascular disease. Even secondhand smoke isn’t safe.Exposure to secondhand smoke is correlated with an increased chance of developing lung cancer, chronic illness, and sickness-related work absences. It’s easy to say, best to stay away.
Minimize Drinking
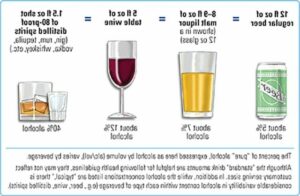
Moderate alcohol consumption has been shown to reduce the risk for coronary heart disease by raising the drinker’s levels of high-density lipoprotein (HDL) cholesterol. Higher levels of HDL cholesterol help to keep the arteries free of blockage. Moderate alcohol consumption is defined as a 12-ounce serving of beer, a 5-ounce glass of wine, or a 1.5-ounce gin, vodka, rum, or scotch. However, chronic alcohol abuse weakens the immune system, promotes the formation of fat deposits on the heart muscle, impairs judgment, and makes it harder for drinkers to focus on multiple stimuli.
These three big categories will help you establish a healthy lifestyle. Keep in mind that these are all physical changes you can make. However, you can also make mental changes to increase your well-being. Here are 10 other little habits to get into:
- Be physically active
- Be spiritual
- Nurture relationships
- Find meaning
- Be mindful
- Commit to your goals
- Go with the flow
- Be thankful
- Practice kindness
- Savor joys
Straub, R. O. (2017). Health psychology: A biopsychosocial approach. New York: Worth, Macmillan Learning.

 Often regarded as the
Often regarded as the